People with type 2 Diabetes can be treated with Tablets at least initially. There are certain situation like pregnancy when you need to take Insulin. There are different types of tablets available and they work in different ways.
Sometimes we use a combination of tablets to get better effect. There are other tablets with a different mode of action are currently undergoing clinical trials.
Can everybody with Diabetes take tablet treatment?
Tablet treatment is for people with type 2 Diabetes except for certain situation like pregnancy when you need to take Insulin.
Also, Insulin is needed during surgery, severe infection and for some reason or other you are not able to eat. Insulin is a must for people with type 1 Diabetes; they should not take the tablet.
When is the right time to start tablet?
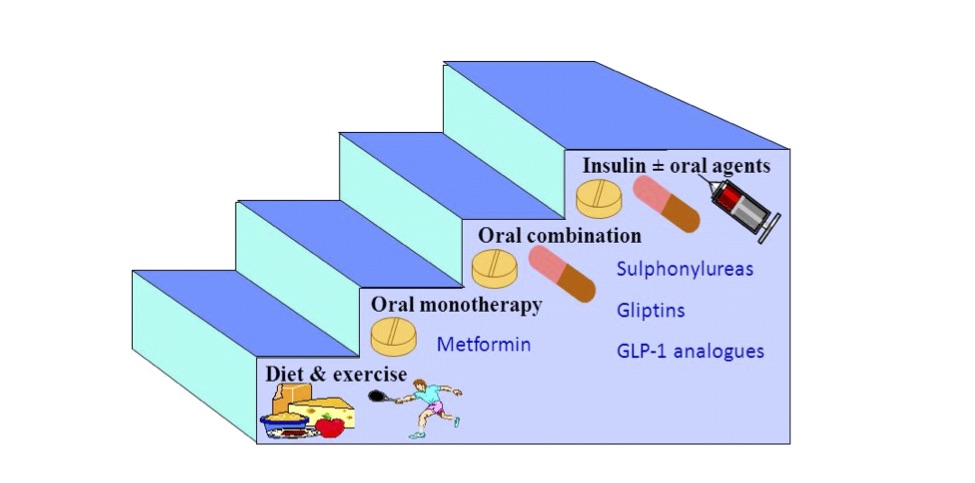
After diagnosis of type 2 Diabetes is confirmed, it is advisable to try diet for some time. This is mainly to make you realise the nature of food you should take and the ones you need to avoid.
After this trial period of diet only, you should check your diabetes control and if the control is not acceptable you should start on diet plus tablet treatment.
Are all the tablets same?
Certainly not. There are different groups of Diabetes tablets available. To complicate the issue further, several companies in India make the same medicine.
So same group or subgroup medicine is available in different names, some of them may be in 50 different names.
Please make sure the name in prescription matches the medicine you buy. To confuse the issue further, some company marketed tablets almost sound like Insulin, but they are tablet, not oral Insulin.
What are the different types of tablets available for Diabetes?
| S.NO | Name | Mech of action | Group |
|---|---|---|---|
| 1 | Sulphonylureas | Stimulates insulin secretion from pancreas | Glipizide Glimeperide |
| 2 | Biguanides | Decreases hepatic production of glucose and increases utilisation | Metformin |
| 3 | Glitazones | Insulin sensitisers | Pioglitazone Rosiglitazone |
| 4 | Glinides | Stimulates insulin secretion | Repaglinide Nateglinide |
| 5 | Alpha Glucosidase inhibitors | Inhibits digestive enzyme | Acarbose Voglibose Miglitol |
| 6 | DPP-4 Inhibitors | Increases Insulin and suppresses anti-Insulin hormone called Glucagon | Sitagliptin Saxagliptin Vildagliptin Linagliptin Teneligliptin |
| 7 | SGLT2 Inhibitors | Increases the renal glucose excretion | Canaglifozine Empaglifozine Dapaglifozine Ipreglifozine |
Biguanides: Metformin
Mechanism of action: Reduction in hepatic gluconeogenesis, Reduction in appetite, Inhibition of intestinal absorption of glucose, Increase in insulin mediated glucose utilization in peripheral tissues such as muscle and liver, they help in lowering triglycerides by decreasing the hepatic synthesis of triglycerides.
Dose: Upto 1gm thrice daily, duration of action is 8-12 hrs
Adverse effects: Nausea, Diarrhea, abdominal discomfort and vitamin B12 malabsorption.
Contraindications: Renal failure, hepatic failure and respiratory failure and severe cardiac failure.
Sulphonylureas
Mechanism of action: Sulphonyl ureas are sulphonamide derivatives which stimulate insulin secretion by their action on the pancreatic beta cell.
Available agents:
- Glibenclamide: Duration of action is 16-24 hrs. Dose: 2.5 -20mg/day.
- Glipizide: Duration of action is 8-12hrs. Dose: 2.5 – 20mg/day.
- Glimeperide: Duration of action is 16-24hrs. Dose:1-8mg/day.
Adverse effects: Hypoglycaemia is a common side effect; older agents like glibenclamide can produce prolonged hypos. Weight gain and Hypersensitivity reactions (including Stevens – Johnson syndrome).
Contraindications: Renal insufficiency, Hepatic insuffiency, Type 1 Diabetes, Diabetic ketoacidosis.
Meglitinides
Meglitinides are non sulphonylurea insulin secretagogue.They stimulate insulin secretion.
Available agents:
- Repaglinide: 0.5mg – 4mg, three times a day
- Nateglinide: 60mg – 180mg thrice a day. They are not very potent and are rather expensive. They are contraindicated in hepatic insufficiency.
Thiazolidinediones
Thiazolidinediones also known as glitazones, they improve insulin sensitivity.
Available agents:
- Pioglitazone: 7.5mg, 15mg & 30 mg once daily.
- Rosiglitazone: 8mg in two divided doses.
Adverse effects: Weight gain, Fluid overload, pedal edema, Hepatotoxicity.
Contraindications: Ischaemic heart diseases, Hepatitis, Volume overload states.
Alpha Glucosidase Inhibitors
Mechanism of action: They inhibit the digestive enzyme and delay the absorption of carbohydrates.
Available agents:
- Acarbose inhibits pancreatic amylase. Dose 50 – 150mg
- Voglibose Dose: 0.2-0.3mg/day with each meal.
- Miglitol Dose: 25mg thrice daily.
Contraindications: Chronic intestinal diseases, Diabetic ketoacidosis, inflammatory bowel disease, intestinal obstruction.
DPP-4 Inhibitors (Dipeptidylpeptidase inhibitors)
Mechanism of action: Glucose mediated insulin secretion, inhibition of glucagon secretion and stimulates insulin biosynthesis.
Available agents:
- Sitagliptin Dose: 100mg once daily
- Saxagliptin Dose: 2.5 – 5mg once a day
- Vildagliptin Dose: 50mg once/twice daily
- Linagliptin Dose: 5mg once daily
Adverse effects: URTI, Nasopharyngitis, headache, Hypoglycemia with Sulphonyl ureas.
Contraindicated in children, pregnant and lactating women.
SGLT2 Inhibitors
Mechanism of action: These are new class of medications which lower blood sugar levels by increasing the renal glucose excretion.
Available agents:
- Canaglifozine Dose 100 -300mg/day
- Empaglifozine Dose 50mg/day
- Dapaglifozine Dose 2.5 -50 mg/day
- Ipreglifozine Dose 100mg/day.
Adverse effects: Increase urinary frequency, UTI, Vulvovaginal infection, Nausea, constipation and diarrhea.
When should I take tablets, before or after food?
Some tablets should be taken before and some after food. Some tablets even should be taken with the first bite of food, because that is the time they work best. This is very important and you should make this clear from your doctor. If it is before, correct time is around 30 minutes before food.
How do they work?
Different tablets work in different ways. Some stimulate the pancreas to produce more Insulin, some tries to help body’s Insulin to work more efficiently while some others do not allow sugar to be absorbed from the stomach. Few tablets work in more than one way.
Can I combine different tablets together?
Yes, if needed. Generally the rule of thumb is to try the maximum dose or maximum tolerated dose of one group and then combine the second tablet from a different group so that they can work together. But now-a-days we are using combination tablet even from the beginning.
Do they have side-effects?
Every medicine available in the market can have side-effects, so does Diabetes tablets. It is very important that you tolerate the medicine, because if you do not tolerate you can not take them for a long time.
If you have side-effects, you must make sure that is due to the tablets before stopping.
Interestingly, some of the side-effects like indigestion, belching, loose motion with Metformin group of tablet disappear over time, so they should be started with a small dose to get adjusted with your system. Once adjusted, the dose can be increased.
Once started, do I need to take them for life?
This all depends on your Diabetes. If your Diabetes is very well controlled, you may try only with diet. If that is fine, why not to control your Diabetes only with diet and life-style measures.
But if you see, your control is not good with diet alone, you must accept that your body needs medicine and you should start again.
Remember, there is a genuine chance, over the time your requirement of medicine is going to go up as type 2 Diabetes worsens with time.
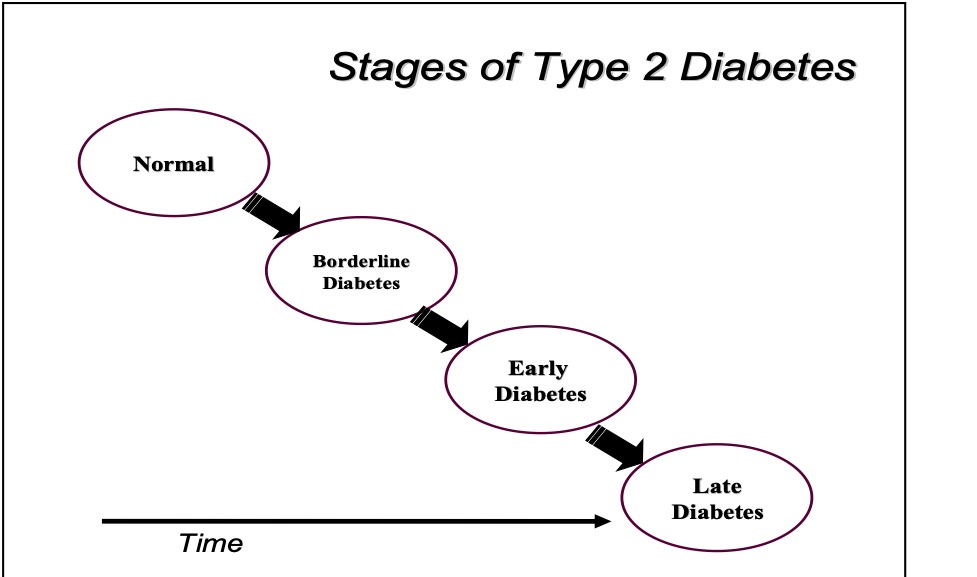
Initially, I was controlled with tablets, but despite doing the same things my sugar is uncontrolled?
This is a very common question we face in our daily practice. The reason for telling, again and again, is that modern research established clearly that Diabetes never remains the same.
The time for this worsening is different for different people. This is neither a fault of yours nor your doctor’s.
If you have looked after yourself very well, it is very likely Diabetes will worsen slowly and the opposite is true as well. So, if you find despite doing the same thing your control is slipping, you should modify the treatment.